CASE OF 47 YEAR OLD WOMAN WITH DYSARTHRIA
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.
Here we discuss our individual patient's problems through a series of inputs from an available global online community of experts with an aim to solve those patient's clinical problems with collective,current,best evidence based inputs.
This e-log book also reflects my patient centered online learning portfolio and your valuable inputs in the comment box is welcome.
Neha Tipparaju
9th Semester, Roll no. 100
CASE OF 47 WOMAN WITH DYSARTHRIA
Patient is a 47 year old housewife, living in Nalgonda.
Timeline of events:
8 years ago, she had 2-3 events where she would have a staring look and not respond to any commands. This episode would last for 5 to 10 minutes.
When she went to a hospital for this, where she was diagnosed as hypertensive. No scanning was done, but since then, she has been taking Amlodipine tablet daily.
6 years back, she had abnormal uterine bleeding and menorrhagia. She underwent hysterectomy (maybe for fibroids). When the stitches weren't healing, she was tested and diagnosed as diabetic. Since then she has been on tab glimiperide and metformin.
Patient was apparently asymptomatic 15 days back when she fell on a wet floor and hurt her left side of abdomen.
The next day she went to an RMP doctor for the pain and received some tablets which she used for 2 days but did not get relief.
Hence she went to an MBBS doctor at Chanduru where he did a scan and said that there is no involvement of bone and the pain was due to involvement of muscle and gave her a pain killer injection, in the left gluteal region. She then had an episode where she woke up, unable to speak and walked out of the hospital where she was found by the attendor. She subsequently went on to complain of:
Slurring of speech which was sudden in onset, developed 1 day back, the speech is not fluent and there is change in voice .
Double vision which was sudden in onset,since 1 day and present when seen with both the eyes, but when seen with either eye closed there is no double vision .
Diminision of vision- in the right eye which was sudden in onset, since 1 day.
Dizziness when the patient is standing or walking, which is sudden in onset since 1day and feels that the patient herself is moving, because of which she's unable to walk without support.
Numbness and swelling of tongue which was sudden in onset since 1 day.
No h/o seizures, headache, vomiting, diarrhoea, no difficulty in deglutition.
Past history:
There were no similar complaints in the past.
Personal history:
Diet: Mixed
Appetite:Normal
Sleep:Adequate
Bowel and bladder:Regular
No known allergies or addictions
General Examination:
Patient is conscious, coherent and cooperative. Oriented to time, place and person.
Moderately built and nourished
Pallor was noticed
No icterus
No cyanosis
No clubbing
No generalized lymphadenopathy
No generalized edema

Vitals:
Temperature:afebrile
PR:77bpm
BP:130/80mmhg
RR:19/min
PO2:99%
GRBS: 229mg/dl
Systemic examination:
CNS:
Oriented to time,place,person
Memory : recent, remote intact
Speech: slurred, dysarthria present. Was unable to speak clearly words like, 'Amritsar'
Cranial nerves:
1-intact
2-diplopia in binocular vision
monocular vision:normal
colour vision:normal
3,4,6- normal(no restriction of movements of eye). Horizontal nystagmus is seen.
5-normal( muscles of mastication+sensations of face) No jaw jerk
7-Normal, wrinking seen, able to blow up cheeks
8- Normal hearing
9,10,11,12-normal. Gag reflex is normal.
Motor-
Tone -normal
Power
4-/5 in b/l lowerlimbs
5/5 in upper limbs
Reflexes :
Biceps:b/l:2+
Triceps:2+
Supinator 2+
Knee:3+
Ankle: 2+
Plantars: Very less response
Sensory: crude touch, pain ,temp, fine touch, joint position, proprioception are normal in all dermatomes
Cerebellum examination:
Able to do finger nose test.
No dysdiadokinesia
No rebound tenderness
Nystagmus present- gaze evoked , horizontal more on right gaze with fast component towards the right, and seen with upward gaze- vertical upbeat and downbeat +.
Gait: slow paced, swaying on both sides. Hesitancy to walk and turn.
CVS: S1 S2+ no murmurs heard.
Respiratory system- Bilateral air entry+ ,normal vesicular breath sounds-heard
Abdominal: Soft, non tender, no distension, umbilicus is central and inverted,no scars, no sinuses, hernial orifices free.
Provisional diagnosis:
Anaphylaxis causing swollen tongue (?)
Acute infarction in the left pons
Hence speech impairment secondary to stroke (?)
Spastic dysarthria (?)
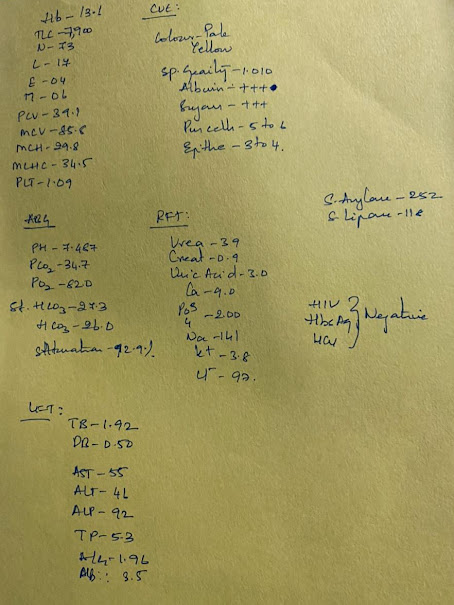
Investigations:

MRI scan showed:

Management:
Tab. ECOSPRIN 150mg PO/OD
Tab. CLOPIDOGREL 150mg PO/OD
Inj. NPH S/C BD 20U
Inj. HAI 10U-10U-8U
Tab. BPLEX FORTE OD
Patient was advised to continue medication, practice verbal exercises at home and was discharged.


Comments
Post a Comment